
Why Stress Makes You Exhausted. In the Spotlight: Cortisol, HPA Axis Dysfunction and Circadian Rhythm
Why You Feel So Tired When You’re Stressed
Most people think of stress as a mental state – worry, pressure, overwhelm. But physiologically, stress is a full‑body event, and your main conductor is a hormone called cortisol.
Cortisol is not the villain it’s often made out to be. In the right amounts, at the right times, it wakes you up in the morning and keeps you alert, fuels your brain, stabilises blood sugar and helps you respond to life’s demands.
The problem starts when stress becomes long-lasting. When pressure is constant, your stress system (or stress response, or the hypothalamic‑pituitary‑adrenal (HPA) axis) stops behaving like a finely tuned thermostat and starts acting more like a stuck accelerator. The result is a body that feels permanently “on” and a brain and nervous system running on fumes.
That is why you can feel wired and tired at the same time.
Cortisol 101: Your Stress And Energy Hormone
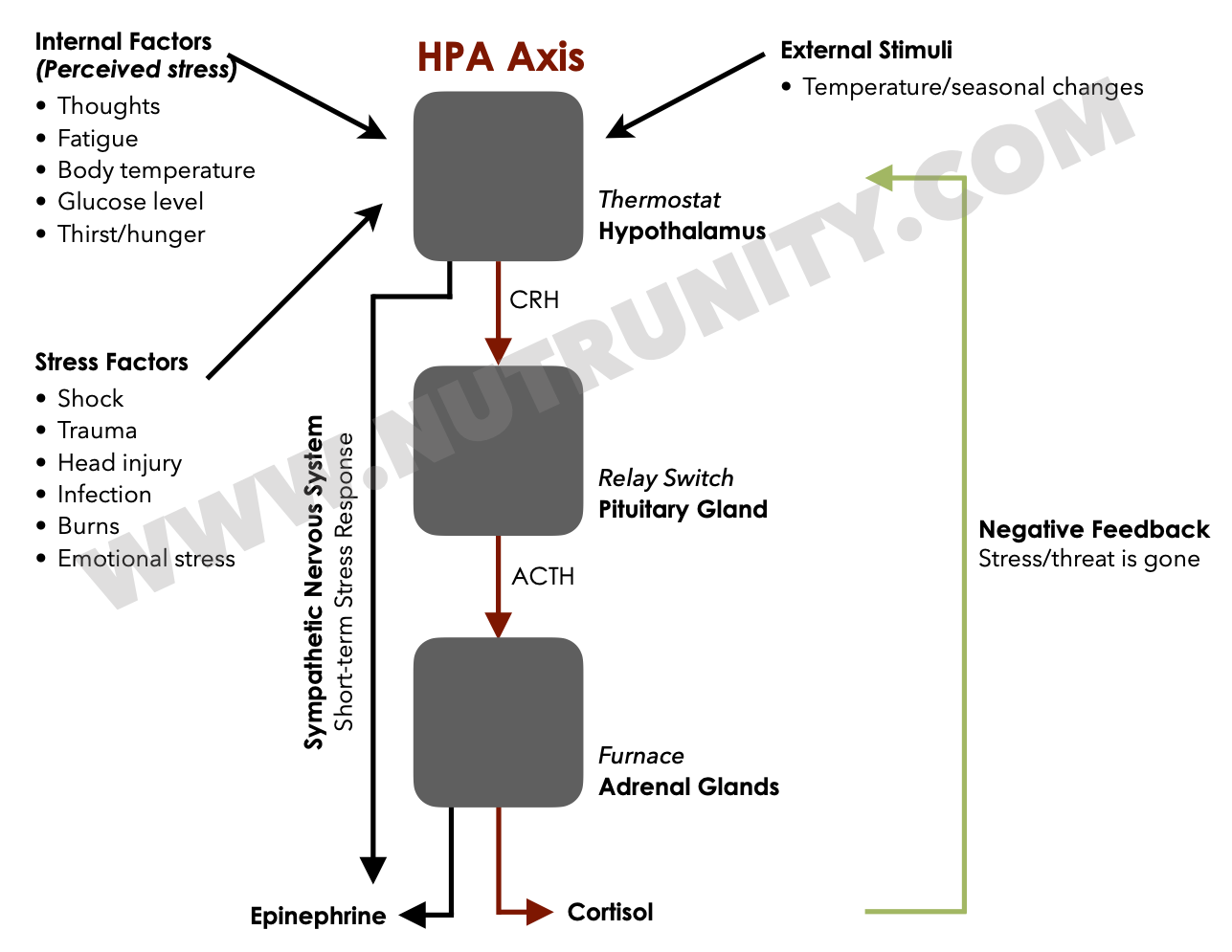
Cortisol is produced by your adrenal glands under instruction from the brain via the HPA axis. In a healthy rhythm:
Cortisol peaks in the early morning to help you wake up, think clearly and mobilise energy. Without it, you couldn’t get out of bed.
It then gradually declines across the day, reaching its lowest point in the evening, and levels are negligible at night, so you can sleep.
In an acute stressor (e.g., a deadline, an argument, a near‑miss on the road), cortisol immediately, but temporarily, rises to:
Release glucose from the liver for a quick burst of energy (remember the stress response, also known as “fight-or-flight” mode, is exactly that. It monopolises energy resources so you can fight back or run as fast as possible to escape from danger)
Increase blood pressure and heart rate (nutrients and large amounts of glucose need to reach muscle tissue very fast)
Sharpen focus and reaction speed (so you can outsmart the predator or find the quickest route of escape)
Once the stressor ends, cortisol should return to baseline. This rise‑and‑fall is designed for short bursts — not for modern life’s relentless alerts and invisible threats.
How Chronic Stress Breaks Your Cortisol Rhythm
When stress is frequent or unrelenting (for example, overwhelming workload, tight deadlines, financial strain, caregiving, unresolved trauma, chronic sleep loss and/or inflammation/infection), the HPA axis adapts in maladaptive ways.
Patterns we see in practice include:
1. Chronically high cortisol (the “hyper” phase)
Elevated or flattened‑high cortisol across the day.
Difficulty winding down at night (feeling “wired-but-tired”).
Fragmented or light sleep, early waking (you sleep with one eye open, as your brain senses danger is imminent).
Feeling anxious, highly irritable or jumpy, yet deeply fatigued, feeling drained.
High cortisol is costly:
It burns through glucose and lean muscle, then drives cravings for quick sugars and stimulants (leading to severe loss of muscle and bone mass).
It disrupts thyroid function and sex hormones, adding another layer of exhaustion (while also affecting energy. Mitochondria are very sensitive to stress. They are in charge of producing energy, as well as sex hormones).
It suppresses melatonin at night, undermining deep, restorative sleep. (Cortisol works oppositely to melatonin; when the levels of one go down, the other’s go up)
2. Blunted or low cortisol (the “crash” phase)
In some people, especially after prolonged over‑activation, the HPA axis starts to down‑regulate:
Lower total cortisol output (often called “hypocortisolaemia” or HPA axis dysfunction)
Flatter diurnal rhythm (not enough rise in the morning, not enough drop at night)
Profound morning heaviness, “walking through treacle” sensation (remember cortisol is what gets you out of bed)
Heavy reliance on caffeine just to feel vaguely normal
This pattern is seen in a subset of people with chronic fatigue, burnout and long‑standing stress exposure. The system has not “failed”; it has adapted to long‑term overload by turning the volume down, at the cost of your energy, resilience and zest for life.
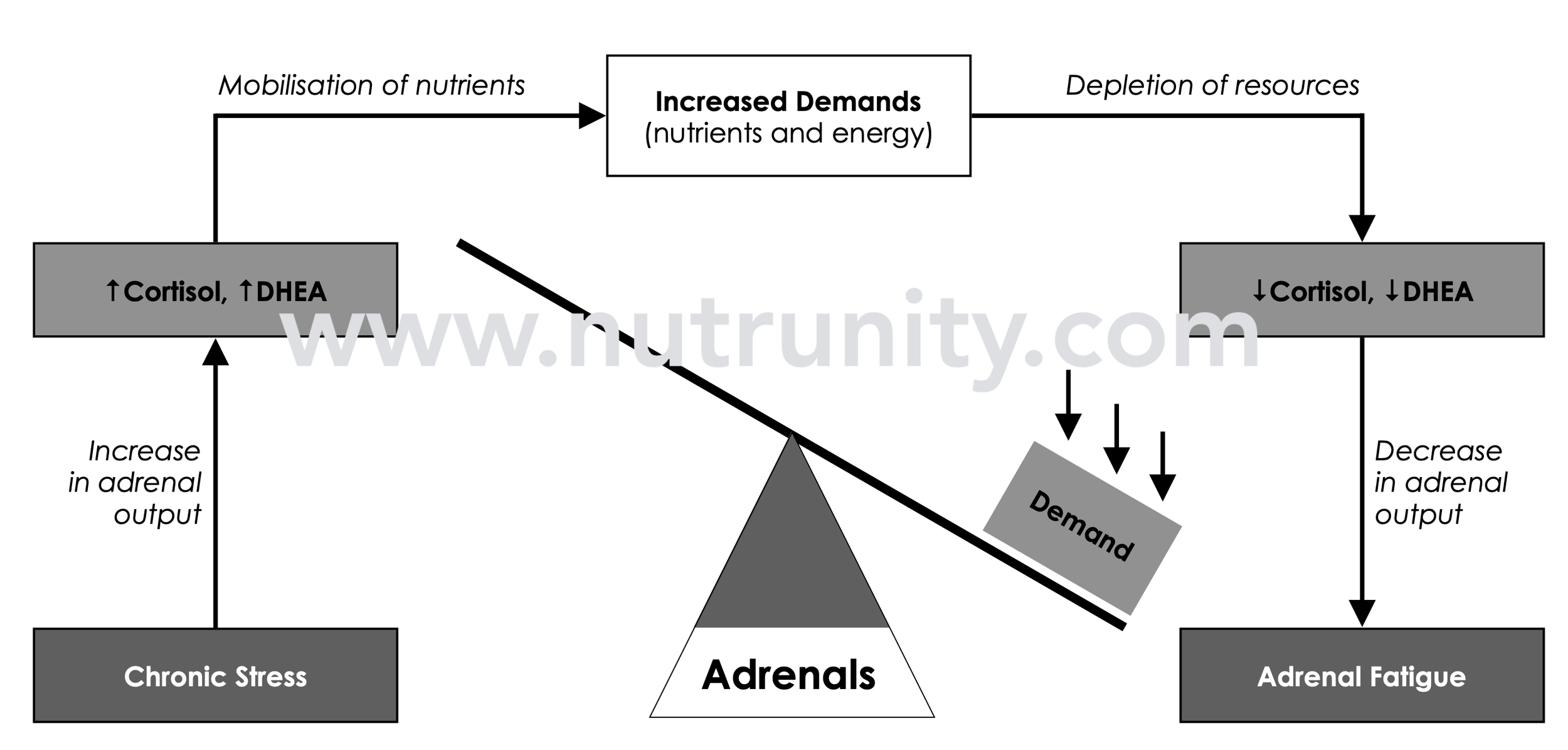
HPA axis dysregulation (commonly known as adrenal fatigue) results from ongoing assaults on the nervous system and depleted resources, leading to fatigue and sleep problems and creating a self-feeding cycle. Illustration by Olivier Sanchez. Extracted from “Energise - 30 Days to Vitality.” All rights reserved.
How Cortisol Controls (And Damages) Your Energy Balance
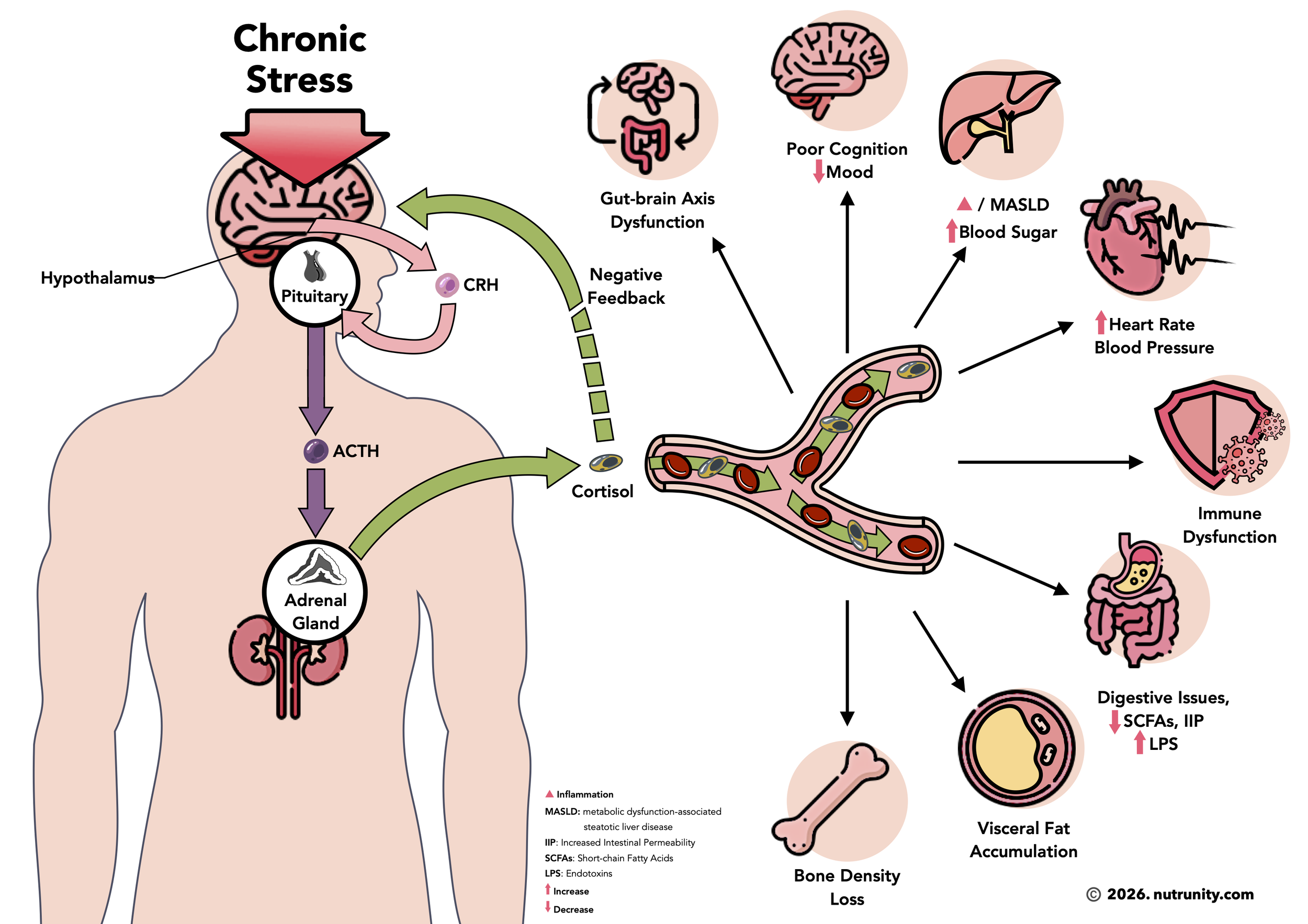
Chronic stress and cortisol dysregulation impact energy on several fronts:
1. Blood sugar and energy crashes
Cortisol mobilises glucose from the liver and tissues to keep your blood sugar up when you’re under threat. Helpful in the short term; damaging when constant.
Persistently high cortisol → frequent glucose release → more insulin spikes → energy crashes and cravings (because insulin is still present in the bloodstream while glucose levels have sharply diminished).
Over time, this pattern contributes to insulin resistance (it’s like setting fire to the cells’ receptor sites. A few burst of cortisol activate their function, too much, and the cell can’t take constant stimulation and switches them off). This pattern also contributes to visceral fat gain and “tired but wired” afternoons.
2. Sleep disruption and circadian chaos
Cortisol and melatonin are dance partners. When cortisol is high late at night, or the daily rhythm is flattened:
It becomes harder to fall asleep or stay asleep.
Deep, slow‑wave sleep (the most physically restorative stage) is reduced, and so is natural healing and repair of the body.
Burnout studies in healthcare workers show a consistent pattern: elevated or misaligned cortisol, suppressed melatonin, and significant sleep disturbance, with downstream fatigue, mood changes and performance issues.
3. Inflammation and immune load
Under normal conditions, cortisol helps regulate immune responses and restrain excessive inflammation (cortisol is anti-inflammatory, which explains why some people feel pain rising in the evening). With long‑term dysregulation:
Tissues may become less responsive to cortisol’s signals (aka glucocorticoid resistance).
Pro‑inflammatory cytokines like IL‑6 and TNF‑α rise.
The result is systemic low‑grade inflammation: aches, pains, brain fog, slower recovery, and a higher risk of autoimmune and cardiometabolic disease.
Inflammation itself is energetically expensive. Your immune system is an enormous energy sink when chronically activated.
4. Mitochondria, muscle and metabolism
Chronic stress alters mitochondrial function, encourages abdominal fat deposition and can promote muscle breakdown, especially when combined with under‑eating or poor protein intake. Excessive intake of caffeine, in addition to blood dysregulation) may also contribute to bone mass loss.
Less functional muscle = lower resting metabolic rate and poorer blood sugar control.
More visceral fat = more inflammatory signalling and hormonal disruption.
No wonder you feel as if your body’s “battery” no longer charges properly.
5. Thyroid dysfunction
Chronic stress doesn’t just drain energy through cortisol and disturb the HPA axis; over time, it can also disrupt thyroid physiology and, in some people, increase the risk or severity of autoimmune thyroid disease.
How stress affects thyroid hormone physiology
Under prolonged stress, the body often downregulates metabolism as a protective mechanism. Below are key patterns that can appear over time.
Reduced conversion of T4 to T3 : Cortisol and inflammatory cytokines can inhibit deiodinase activity, so less T4 is converted into active T3 and more into reverse T3 (rT3), which is metabolically inactive (the body’s handbrake). The person may have “normal” TSH/T4 on paper but feel (hypothyroid) fatigue, weight gain, cold intolerance, low mood, and brain fog.
Blunted TSH secretion dynamics: Chronic HPA activation alters hypothalamic and pituitary signalling. In some individuals, TSH may not rise appropriately despite low tissue T3, which is one reason why stress‑driven low‑T3 pictures are sometimes missed if only TSH is checked.
Impact on thyroid receptor sensitivity: Ongoing inflammation and oxidative stress can reduce thyroid receptor sensitivity at the tissue level, so even normal circulating hormone levels can feel “weak” clinically.
Stress, autoimmunity and thyroid antibodies
The relationship between stress and autoimmune thyroiditis (Hashimoto’s, Graves’) is complex and bidirectional, but several themes emerge.
Immune dysregulation: Chronic cortisol dysregulation (initially high, then sometimes low) impairs normal immune balance and barrier function (gut, blood–brain), increasing the likelihood of loss of tolerance. That can contribute to the development or flaring of thyroid autoantibodies (TPO, Tg, and in Graves’, TSH‑receptor antibodies) in genetically susceptible people.
Triggering and flares: Major life stressors (bereavement, divorce, overwork, trauma, infection) are frequently reported around the onset or flare of autoimmune thyroid disease. Mechanistically, stress can increase intestinal permeability and dysbiosis, thereby feeding immune activation; raise inflammatory mediators that promote autoantibody production; and alter regulatory T‑cell (Treg) function, reducing immune “braking.”
Clinical pattern: Someone may move from “subclinical autoimmunity” (positive antibodies with normal labs) into overt hypo‑ or hyperthyroidism after a period of intense or cumulative stress.
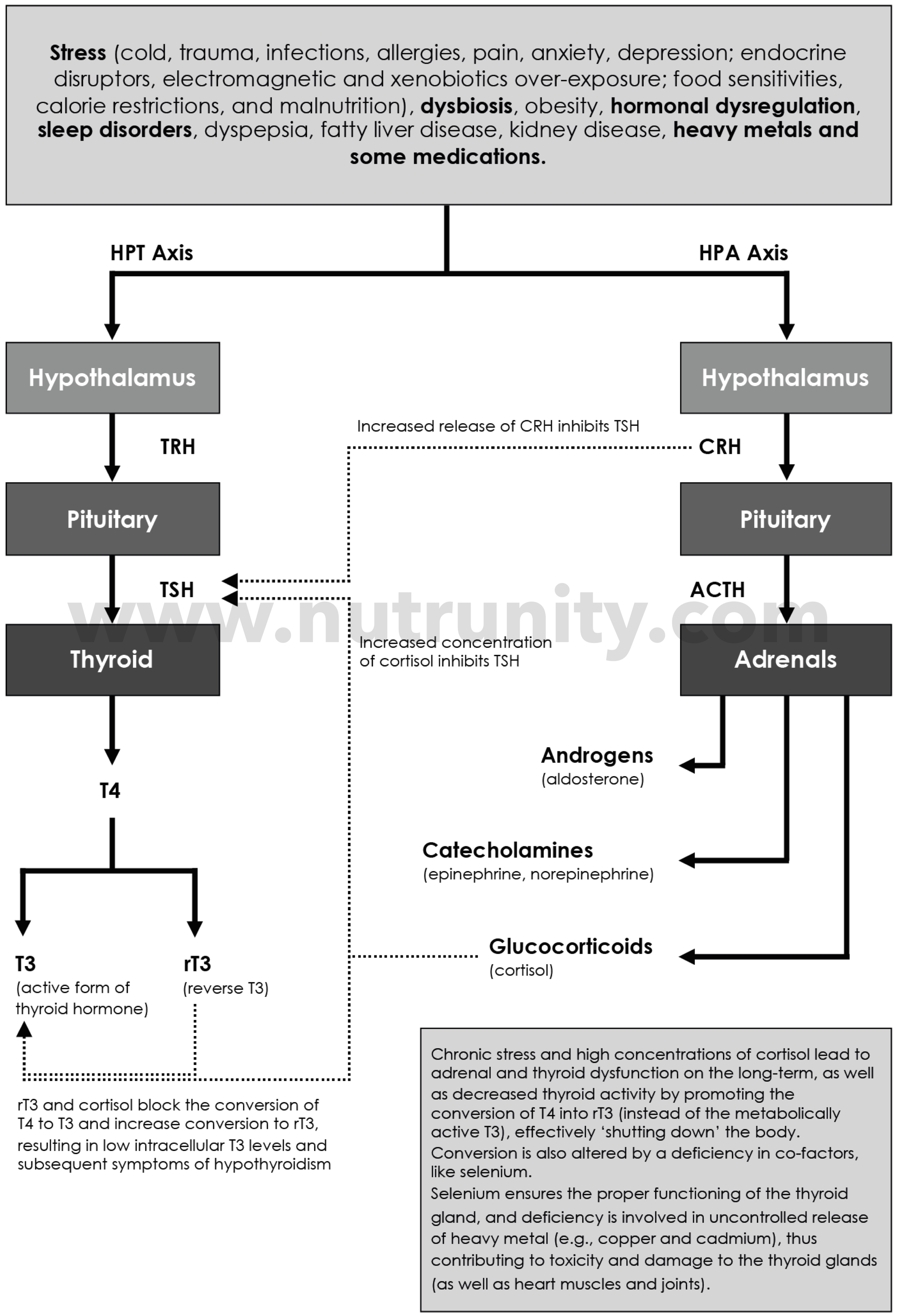
rT3 and Hyperactivation of the HPA Axis. All systems in the body are interconnected, and chronic stress disturbs them all. Illustration by Olivier Sanchez. Extracted from “Energise - 30 Days to Vitality.” All rights reserved.
Why You’re Still Exhausted Even When You Sleep
This is the most common complaint I see in practice:
“I’m sleeping 8 hours, but I wake up tired and desperate for coffee first thing in the morning just to function. I feel useless without my coffee.”
If your HPA axis is dysregulated, sleep quantity is not the whole story. You can tick the 7–8 hour box yet:
Have cortisol too high at night → light, non‑restorative sleep.
Have cortisol too low in the morning → poor alertness and slow mobilisation.
Have chronic inflammation and mitochondrial dysfunction that make rest less efficient.
Your thyroid function may also be disrupted by chronic hypercortisolaemia.
This is why simply “going to bed earlier” often doesn’t fix deep fatigue. The rhythm and regulation of cortisol and the nervous system must be addressed.
Cortisol + Stress Response System
Practical Steps To Help Rebalance Cortisol And Energy
There is no magic supplement that “fixes cortisol”, but there are evidence‑informed levers you can pull.
1. Restore your circadian rhythm
Get morning daylight within 30–60 minutes of waking to support a healthy cortisol awakening response.
Keep a consistent sleep–wake schedule, even at weekends.
Dim lights and reduce screens 60–90 minutes before bed to allow cortisol to drop and melatonin to rise.
In the morning, use your journal to set the tone for the day by writing down your intentions for the day, listing them by priority, and choosing up to 3 affirmations. In the evening, reset the stress response with journaling to jot down what destabilised your emotions during the day, what made you smile or even happy, and before closing your journal, write down three things for which you feel grateful. These must be positive.
2. Eat to stabilise blood sugar
Include protein, healthy fats and fibre at each meal to avoid sharp glucose swings. Supplement with digestive enzymes if under overwhelming stress.
Avoid relying on caffeine and sugar as primary energy tools; they destabilise cortisol and insulin by creating blood sugar roller‑coasters, with extremely stressful crashes.
3. Use stress strategically, not constantly
Build deliberate “off” time into your day: micro‑breaks, breathing practices, gentle movement. Disconnect from devices as soon as you arrive home. If you bring work home, ensure it is in an office or space other than the bedroom or living area. Make clear pauses before dinner, and keep devices off the table. After dinner, it is your me-time. No more work allowed, no more checking emails. It is time to unwind and give your brain the rest it needs and deserves.
Swap some high‑intensity training for restorative movement (walking, yoga, mobility) if you’re already exhausted; intense exercise is a stressor too. Individuals with a strong constitution find it hard to relax if they are not completely exhausted. If this is you, consider gentle exercises, followed by stretching. Do not exercise too close to bedtime to allow your body temperature to drop. Without it, you may struggle to fall asleep.
4. Support the nervous system biochemically
Magnesium, B‑vitamins, vitamin C, omega‑3s and adequate protein are foundational for HPA axis resilience and neurotransmitter balance. A calm supplement complex should also be considered (which may include any of the following: Lemon balm, L-theanine, Holy basil, Saffron (Crocus sativus stigma), Rhodiola, (soy-free) Phosphatidylserine, Magnesium bysglycinate (100-300mg), Cordyceps, and Schisandra).
Any supplementation should be targeted, not random. Ideally based on a full history and, where appropriate, testing. Avoid supplementing without supervision to prevent unwanted and severe side effects.
5. Address hidden stressors
Remember that your brain doesn’t distinguish between:
Emotional stress (conflict, worry, perfectionism)
Physiological stress (gut inflammation, infections, blood sugar crashes
Environmental stress (light at night, shift work, toxins)
Made-up or anticipatory stress (anxiety, fear of the unknown, feeling of impending doom, doomscrolling)
If you focus only on mindset while ignoring gut issues or circadian disruption, your cortisol may remain dysregulated.
When To Seek Professional Help
If you recognise yourself in this description (chronic fatigue, wired‑tired evenings, energy crashes, feeling like a stranger in your own body), you may be dealing with a pattern of HPA axis dysfunction, not mere “busyness.”
This is where a comprehensive, integrative assessment becomes powerful:
Mapping your symptoms against cortisol rhythm, nervous‑system state, sleep and metabolic markers.
Identifying which stresses (emotional, nutritional, environmental, infectious) are most relevant for you.
Designing a phased, realistic plan that honours your physiology rather than fighting it.
Don’t guess and do it alone, trusting Dr Google and ChatGPT blindly.
A Different Way To Relate To Your Energy
Think of cortisol as both your fuel‑mobiliser and your stress barometer. When it is balanced, you wake with energy, respond flexibly to life, and wind down at night. When it’s dysregulated, your nervous system is in survival mode, and nothing else matters, not your digestion or your immunity. Everything from now on is done on your behalf to keep you safe, even if that means becoming more isolated and not finding joy in activities that used to make you happy.
You don’t have to live permanently in that survival mode.
If you’re ready to stop guessing, stop blaming yourself, and start working with your biology, this is the moment to take a different kind of step.
→ Book a comprehensive stress and fatigue programme
In clinic, we use the latest evidence on HPA axis function, nervous‑system regulation and functional testing to help clients move from wired‑and‑tired to grounded, energised and clear‑headed. Around 95% of the people I see arrive in a state of disproportionate overwhelm, chronic stress and persistent fatigue; they leave with a map, a plan and, crucially, the felt sense that their energy can be rebuilt.
The clock will keep ticking regardless. The real question is whether you want to continue running on empty, pushing against the wall, or learn how to restore a rhythm that makes your life feel sustainable, spacious and fully lived.
References:
Andreadi, A., Andreadi, S., Todaro, F. et al. (2025). Modified Cortisol circadian rhythm: The hidden toll of night-shift work. International Journal of Molecular Sciences. 26(5), 2090. doi:10.3390/ijms26052090
Chourpiliadis, C., Aeddula, NR. (2023). Physiology, Glucocorticoids. Treasure Island (FL): StatPearls Publishing. PMID: 32809732.
Dunlavey, CJ. (2018). Introduction to the hypothalamic-pituitary-adrenal axis: Healthy and dysregulated stress responses, developmental stress, and neurodegeneration. Journal of Undergraduate Neuroscience Education. 16(2), R59-R60.
Herman, JP., McKlveen, JM., Ghosal, S. et al. (2016). Regulation of the hypothalamic-pituitary-adrenocortical stress response. Comprehensive Physiology. 6(2), pp. 603-621. doi:10.1002/cphy.c150015
Leistner, C., Menke, A. (2020). Hypothalamic-pituitary-adrenal axis and stress. Handbook of Clinical Neurology. 175, pp. 55-64. doi:10.1016/B978-0-444-64123-6.00004-7
Nunez, SG. Rabelo, SP. Subotic, N. et al. (2025). Chronic stress and autoimmunity: The role of HPA axis and cortisol dysregulation. International Journal of Molecular Science. 26(20), 9994. doi:10.3390/ijms26209994
Papadopoulos, AS., Cleare, AJ. (2011). Hypothalamic-pituitary-adrenal axis dysfunction in chronic fatigue syndrome. 8(1), pp. 22-32. doi:10.1038/nrendo.2011.153
Rensen, N., Gemke, RJ., van Dalen, EC. et al. (2017). Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database of Systematic Reviews. 11(11), CD008727. doi:10.1002/14651858.CD008727.pub4
Ring, M. (2025). An integrative approach to HPA axis dysfunction: from recognition to recovery. American Journal of Medicine. 138(10), pp. 1451-1463. doi:10.1016/j.amjmed.2025.05.044
Sheng, JA., Bales, NJ., Myers, SA. et al. (2021). The hypothalamic-pituitary-adrenal axis: Development, programming actions of hormones, and maternal-fetal interactions. Frontiers in Behavioural Neuroscience. 2021 Jan 13;14:601939. doi: 10.3389/fnbeh.2020.601939
Tomas, C., Newton, J., Watson, S. (2013). A review of hypothalamic-pituitary-adrenal axis function in chronic fatigue syndrome. ISRN Neuroscience. 2013, 784520. doi:10.1155/2013/784520
Ungurianu, A., Marina, V. (2025). Melatonin and cortisol suppression and circadian rhythm disruption in burnout among healthcare professionals: A systematic review. Clinical Practice. 15(11), 199. doi:10.3390/clinpract15110199