
How Ultra‑Processed Foods Wreck Your Gut (And Show Up on the Bristol Stool Chart)
You don’t need a fancy test to see what ultra‑processed manufactured food products (UPFs) are doing to your gut; your stool is already reporting back every single day. A UPF‑heavy diet doesn’t just change your weight or blood sugar; it forces shifts in your microbiome, irritates your intestinal lining and shows up as bloating, pain, urgency or constipation long before blood tests look “abnormal.”
How Ultra‑Processed Foods Damage Your Gut Health
UPFs are industrial formulations made mostly from refined ingredients, additives and cosmetic enhancers rather than whole foods. They are typically high in emulsifiers, thickeners, sweeteners, flavour enhancers, colours, preservatives, refined starches, industrial seed oils and trans fats, and low in dietary fibre and polyphenols (antioxidants).
Mechanistic and human data show that high UPF intake is linked to:
Dysbiosis:
Reduced microbial diversity, fewer butyrate‑producers, and overgrowth of pro‑inflammatory/pathogenic species.
Barrier damage (increased intestinal permeability or “leaky gut syndrome”):
Emulsifiers and certain additives alter mucus production, deplete immune cells (secretory IgAs), increase bacterial encroachment, and raise LPS levels (endotoxins), driving low‑grade inflammation.
Altered motility and sensitivity:
These changes contribute to IBS‑type symptoms via the gut–brain axis.
Observational work now links higher UPF intake with increased risk of IBS and other disorders of gut–brain interaction. Clinically, this also translates into a wide range of gut symptoms and stool changes.
Gut symptoms UPFs can provoke
People who rely heavily on UPFs often report:
Bloating and abdominal distension
Excess gas and belching
Cramping or colicky pain
Nausea and early satiety
Heartburn/reflux (from high fat, sugar and additives)
Post‑prandial urgency (urgency after meals) or loose stools
Constipation, diarrhoea, or IBS‑mixed patterns
These patterns reflect the underlying dysbiosis, barrier dysfunction and low‑grade inflammation described in recent reviews. IBS associations are now being captured in the population. Higher UPF consumption is linked to increased risk of IBS and worse symptom severity, especially in women and those with existing gut–brain axis vulnerability.
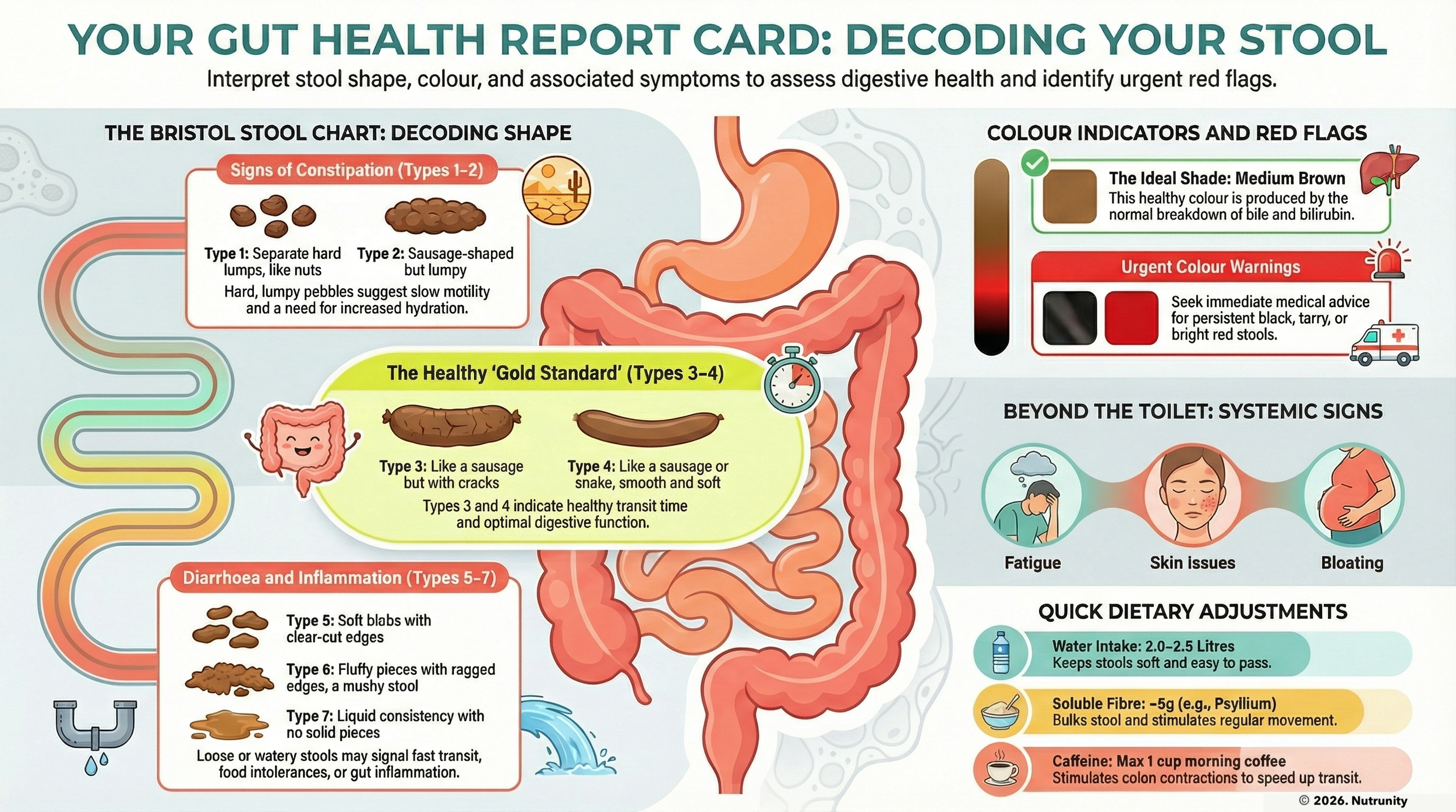
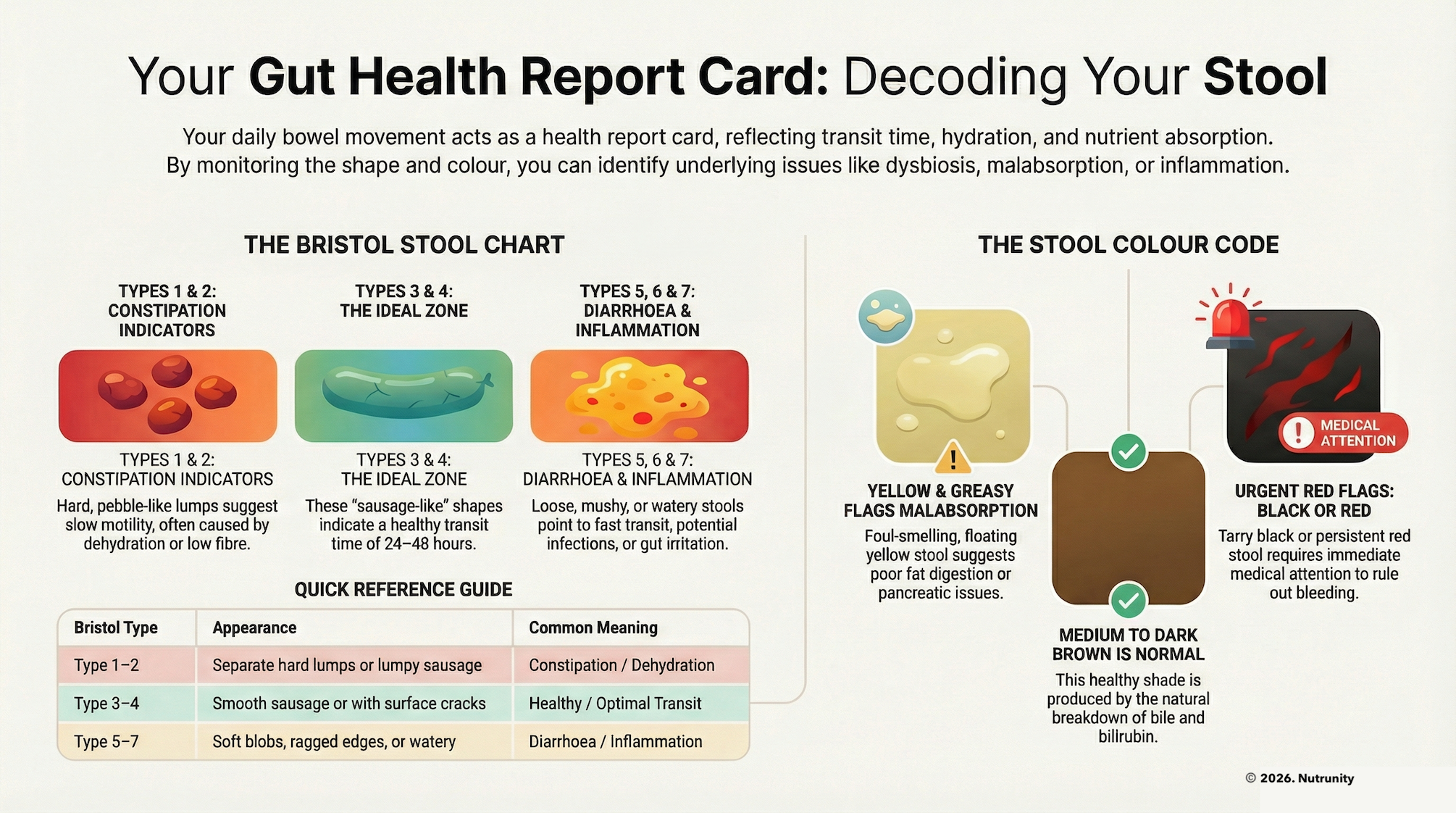
How UPFs affect stool consistency (Bristol Stool Chart)
The Bristol Stool Chart is a validated tool used in gastroenterology to categorise stool form from type 1 (hard pellets) to type 7 (watery). In a stable, well‑fed gut, most people sit around type 3–4. Because UPFs interfere with microbiota, fibre intake, water handling and motility, they tend to push stools to the extremes of the Bristol Stool Chart.
Common patterns
1. Constipation‑leaning pattern (Types 1–2)
This is common in UPF‑heavy diets with low fibre and high salt.
Typical stool pattern:
Infrequent bowel movements (every 2–3 days or less)
Type 1–2 stools (hard, lumpy, pellet‑like)
Straining and a sense of incomplete emptying
Why UPFs push you there:
Very low fibre and resistant starch: Most UPFs are fibre‑poor, which reduces bulk and slows transit.
High salt increases mild dehydration and stool dryness.
Dysbiosis and lower short‑chain fatty acids: Loss of butyrate‑producers reduces motility and mucus production.
Symptoms you may notice:
Bloating, heaviness
Haemorrhoids or fissures from straining
Headaches, “sluggish” feeling after several days without a bowel movement
2. Loose / diarrhoea‑leaning pattern (Types 6–7)
More common when UPFs include a lot of emulsifiers, sweeteners or high‑fructose loads — anything that the body identifies as a hazard or things it doesn’t recognise, which are having a damaging effect on the gut lining or environment.
Typical stool pattern:
Frequent trips to the toilet
Type 6–7 stools: mushy, fluffy, watery
Urgency after meals, sometimes borderline incontinence
Why UPFs push you there:
Emulsifiers and thickeners (e.g., carboxymethylcellulose, polysorbate‑80) have been shown to thin mucus, promote bacterial encroachment, and alter motility, leading to looser stools and low‑grade inflammation in susceptible people (primarily due to depletion of immune cells, such as secretory IgAs).
Sugar alcohols and some sweeteners (e.g. sorbitol, mannitol) pull water into the gut and speed transit.
Pro‑inflammatory dysbiosis: Favouring endotoxin‑producing species can promote secretory diarrhoea‑type symptoms.
Symptoms you may notice:
Cramping pain that improves after a bowel movement
Embarrassing urgency, especially after UPF‑heavy meals
Fatigue from fluid/electrolyte loss
3. IBS‑mixed or highly variable pattern (Types 1–7)
This is the classic “I never know what I’m going to get” scenario.
Typical stool pattern:
Some days type 1–2, other days type 6–7
Occasional type 3–4 mixed in
No predictable rhythm
Why UPFs push you there:
Erratic inputs: Skipped meals followed by large UPF loads, caffeine and alcohol keep motility signalling unstable.
Sensitive gut–brain axis: UPF‑driven dysbiosis and barrier injury heighten visceral sensitivity (a core feature of IBS).
Unstable microbiota: A less diverse, UPF‑exposed microbiome is more prone to “flip” with small triggers (stress, a takeaway, antibiotics).
Research using tools like the “fecograph” (a graphical record of daily stool forms) shows that this variability correlates strongly with IBS subtypes and symptom burden.
4. Gas, mucus and “messy” stools (Types 5–6)
Even when not frankly diarrhoeic, UPF‑heavy diets often produce typical stool patterns:
Type 5–6 stools: soft blobs, ragged edges
Mucus strands on the stool or paper
Strong odour and visible bubbles
Why UPFs push you there:
Mucus layer disruption: Emulsifiers and certain fats interfere with mucus structure, so you see more of it in the toilet. Gluten, an overused additive, also lead to disruptions in the mucous layers and renewal.
Fermentable additives: Stabilisers, refined carbs and sweeteners are rapidly fermented by dysbiotic flora, creating excess gas and altering stool texture.
Symptoms you may notice:
Loud gut noises
A feeling of incomplete emptying
Alternating “OK days” with messy, urgent ones
Why It’s So Important to Notice Stool Changes
The Bristol Stool Chart is a validated proxy for transit time and a practical tool for IBS and gut‑brain disorders. UPF‑driven swings on the chart are an early, visible sign that something is off in the gut ecosystem. If a person increases UPF intake and then notices:
A sudden shift from type 3–4 to persistent type 1–2 (or 6–7), suggesting chronic disturbance of motility, microbiota and barrier integrity.
New urgency, mucus, or pain with defecation
Alternating extremes over weeks
In the longer term, UPF‑linked dysbiosis and inflammation are also associated with a higher risk of depression and faster cognitive decline, underscoring the gut–brain consequences of what’s on your plate.
Tracking your stools over a few weeks, especially as you reduce UPFs and increase whole foods, gives you real‑time feedback on whether your gut is healing or still under stress.
When to Re‑Read “What Your Poop Says About Your Gut Health”
In our recent article “What Your Poop Says About Your Gut Health (And When to Get a Stool Test)”, we explained:
Bristol Stool Chart types and what’s considered normal
Red‑flag symptoms and when to seek medical review
When a stool test (including GI mapping) is appropriate
This new article, specifically on the role of UPFs on stool shape and texture:
Highlights that UPF‑driven swings on the Bristol scale are an early warning sign of dysbiosis/barrier stress.
Encourages you to compare your current stool pattern with the Bristol stool types described in the previous article (click the button above).
Suggests that if changes persist despite reducing UPFs, especially with pain, blood, or weight loss, you should revisit the “When to get a stool test” section and, if needed, seek an immediate medical or personalised assessment.
Use this UPF article as your trigger map, and that stool article as your interpretation guide. Together, they help you:
Identify diet‑related stool changes.
Decide when simple dietary shifts are enough.
Know when persistent symptom patterns, even after removing UPFs, mean it’s time for deeper investigation.
Your poop is one of the most honest reporters you have. If ultra‑processed foods are all over your plate and your Bristol chart is all over the place, your gut is sending you a message.
The question is:
Are you ready to listen?
References:
Cani, PD. (2015). Metabolism: Dietary emulsifiers — sweepers of the gut lining? Nature Reviews. Endocrinology. 11(6), pp. 319-320. doi:10.1038/nrendo.2015.59
Chassaing, B., Koren, O., Goodrich, JK. et al. (20150. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature. 519(7541), pp. 92-96. doi:10.1038/nature14232
Dale, HF., Kolby, M., Valeur, J. (2025). Ultra-processed foods consumption and irritable bowel syndrome: Current evidence and clinical implications. Nutrients. 17(22), 3567. doi:10.3390/nu17223567
Gomes Gonçalves, N., Vidal Ferreira, N., Khandpur, N. et al. (2023). Association between consumption of ultraprocessed foods and cognitive decline. JAMA Neurology. 80(2), pp. 142-150. doi:10.1001/jamaneurol.2022.4397
Lane, MM., Gamage, E., Travica, N. et al. (2022). Ultra-processed foods consumption and mental health: A systematic review and meta-analysis of observational studies. Nutrients. 14(13), 2568. doi:10.3390/nu14132568
Mazloomi, SN., Talebi, S., Mehrabani, S. et al. (2023). The association of ultra-processed food consumption with adult mental health disorders: A systematic review and dose-response meta-analysis of 260,385 participants. Nutritional Neuroscience. 26(10), pp. 913-931. doi:10.1080/1028415X.2022.2110188
Naimi, S., Viennois, E., Gewirtz, AT. et al. (2021). Direct impact of commonly used dietary emulsifiers on human gut microbiota. Microbiome. 9(1), 66. doi:10.1186/s40168-020-00996-6
Panyod, S., Wu, WK., Chang, CT. et al. (2024). Common dietary emulsifiers promote metabolic disorders and intestinal microbiota dysbiosis in mice. Communications Biology. 7, 749. doi:10.1038/s42003-024-06224-3
Pozuelo, M., Panda, S., Santiago, A. et al. (2025). Reduction of butyrate- and methane-producing microorganisms in patients with Irritable Bowel Syndrome. Scientific Reports. 5, 12693. doi:10.1038/srep12693
Rondinella, D., Raoul, PC., Valeriani, E. et al. (2025). The detrimental impact of ultra-processed foods on the human gut microbiome and gut barrier. Nutrients. 17(5), 859. doi:10.3390/nu17050859
Shah, C., Grover, AS., Dhore, P. et al. (2019). Fecograph: A graphical representation of daily stool forms to subtype irritable bowel syndrome in office practice. JGH Open. 3(3), pp. 224-227. doi:10.1002/jgh3.12143
Spiller, AL., da Costa, BGD., Yoshihara, RNY. et al. (2025). Ultra-processed foods, gut microbiota, and inflammatory bowel disease: A critical review of emerging evidence. Nutrients. 17(16), 2677. doi:10.3390/nu17162677
Wu, S., Yang, Z., Liu, S. et al. (2024). Ultra-processed food consumption and long-term risk of irritable bowel syndrome: A large-scale prospective cohort study. Clinical Gastroenterology and Hepatology. 22(7), pp. 1497-1507.e5. doi:10.1016/j.cgh.2024.01.040