
What Your Poop Says About Your Gut Health (And When to Get a Stool Test)
Your daily bowel movement is like a health report card from your gut. Changes in poop colour, shape, texture, or frequency can signal everything from simple dietary tweaks to underlying issues like IBS, dysbiosis, or poor nutrient absorption.
In this guide, we’ll break down the Bristol Stool Chart, common stool red flags, and gut–brain connections. As a registered naturopath specialising in IBS and functional gut health, I’ll show you how to interpret your stool and know when a comprehensive stool test is your next step.
The Bristol Stool Chart: What Shape Reveals About Digestion
The Bristol Stool Chart classifies poop into 7 types based on shape and texture. Types 3–4 indicate healthy transit time (about 24–48 hours through your gut). Types 1–2 suggest constipation or slow motility; 5–7 point to diarrhoea or inflammation.
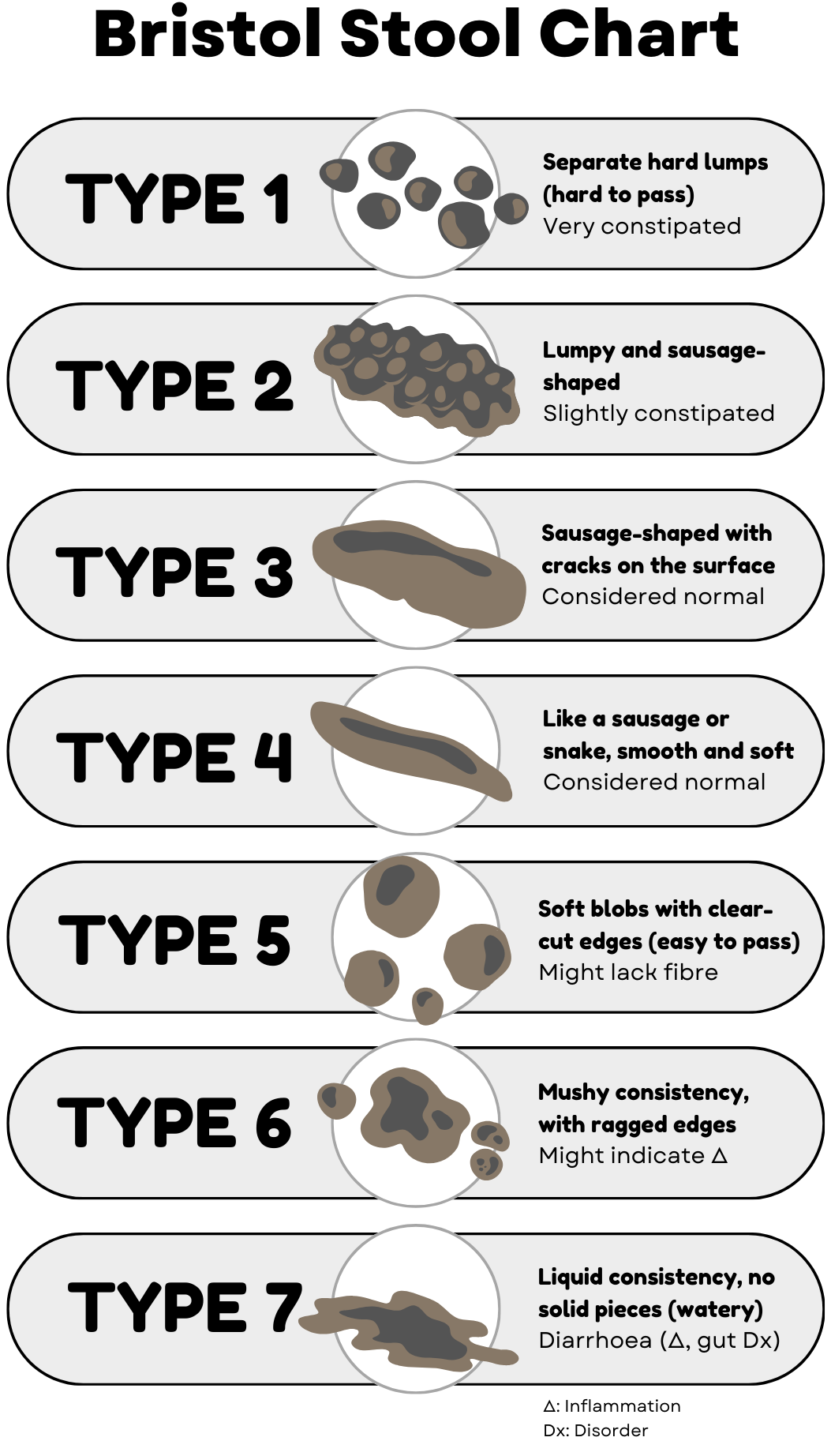
Adapted Bristol Stool Chart. Extracted from “Overcoming IBS” by Olivier Sanchez. All rights reserved.
Track yours for a week and note patterns; it’s the first step to optimising gut health.
What would be considered normal?
Depending on your level of hydration, stress (lack of sleep counts here, too), and food intake (including fibre), your stools may change daily, although they should generally remain consistent. If you are unsure, the Bristol Stool Chart is generally valid and reliable. It may also be useful for children's constipation.
A normal stool should be a type 3 or 4. Type 1–2 indicates constipation; Type 5–7 may indicate diarrhoea
While reliable for extremes, intermediate types are less precise. Even gastroenterologists may not agree on the same score, especially when it comes to diagnosing IBS. Types 2, 3, 5 and 6 stools were less likely to be classified correctly. It is okay if you feel you are between 5 and 6, for example.
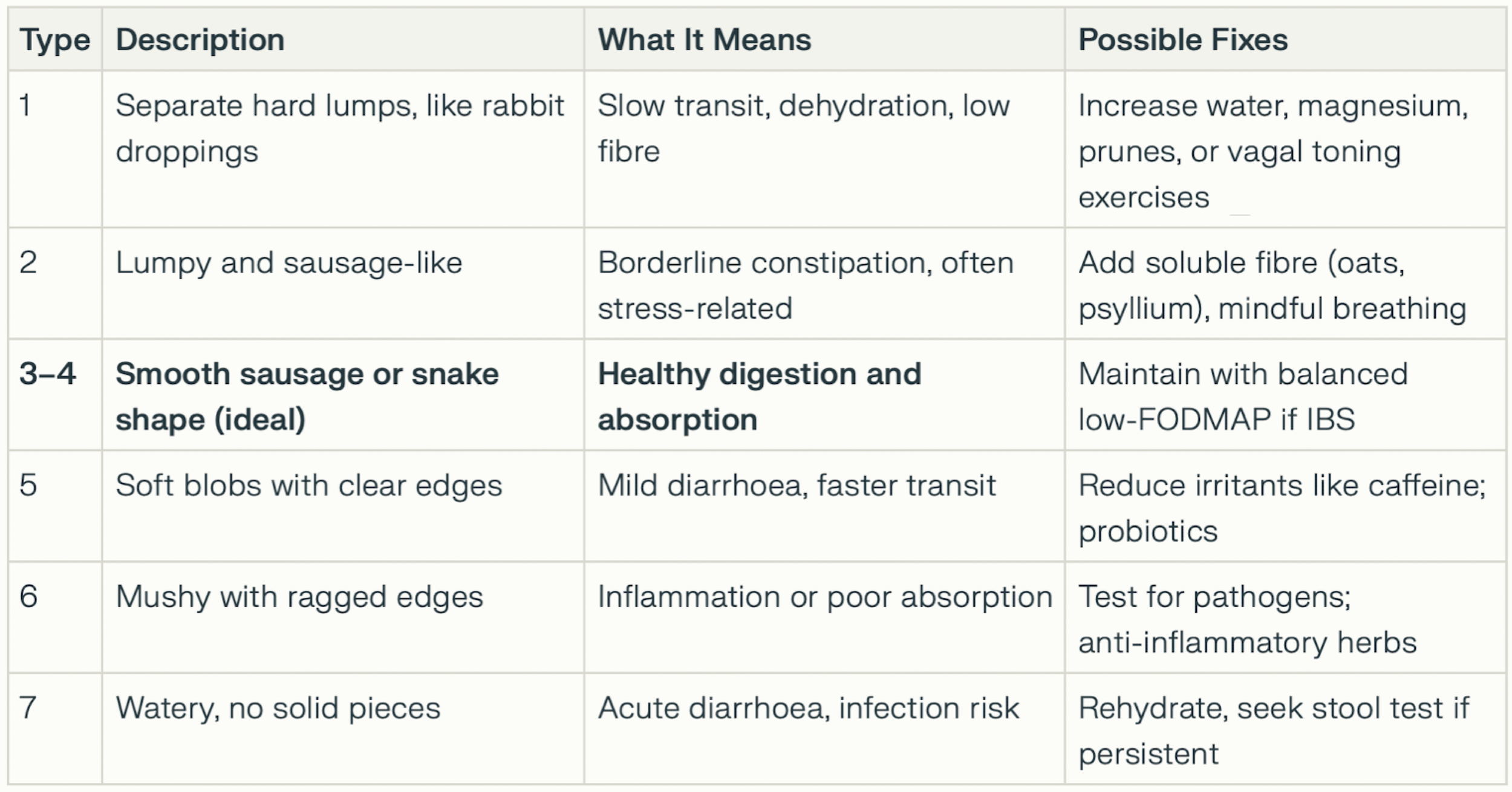
Table 1: of Bristol Stool Chart details and recommendations
Poop Colours: 8 Shades and What They Mean for Gut Health
Healthy stool is medium brown from bile and bilirubin. Abnormal colours often tie to diet but can flag bile issues, malabsorption, or bleeding.
Dark brown: Normal and healthy.
Light brown/pale: Possible low bile (liver/gallbladder) or fat malabsorption.
Green: Fast transit, leafy greens, or bile overload.
Yellow/greasy: Poor fat digestion (pancreas, coeliac, or dysbiosis); often floats and smells foul.
Orange: Beta‑carotene foods or antacids.
Black/tarry: Iron supplements or upper GI bleed (see doctor urgently).
Red: Lower GI bleed, haemorrhoids, or beetroot – persistent red needs checking.
Grey/white: Bile duct issues or meds.
Red flag: If colour changes last >1 week or are accompanied by pain/weight loss, consult a professional immediately.
7 Signs Your Gut Is Unhealthy (Beyond Just Poop)
Poop is linked to the gut–brain axis, immunity, and nutrient status. Watch for these clusters:
Frequent bloating, gas, or alternating constipation/diarrhoea (classic IBS).
Unexplained fatigue or low mood (gut microbes influence 90% of serotonin).
Skin issues like eczema or acne (leaky gut marker).
Food intolerances worsening over time.
Poor sleep or high stress (vagus nerve dysfunction).
Nutrient deficiencies despite diet (e.g. low B12, iron from malabsorption).
Frequent infections (70–80% of immunity is gut‑based).
These often stem from dysbiosis, SIBO, or methylation issues, all of which are detectable through stool analysis.
Can Diet Affect Your Stool Shape and Form?
Yes, diet directly influences stool shape, texture, and transit time because stool is 75% water and contains undigested food fibres, gut bacteria, and dead cells.
Here’s how key dietary factors shift your Bristol Stool Chart type, with practical fixes for better gut motility and IBS management.
Water: The Foundation of Soft, Passable Stool
Healthy stool contains 70–80% water, which your colon absorbs and regulates for easy passage. Dehydration thickens stool into hard Type 1–2 lumps (constipation), slowing motility and straining the vagus nerve.
Fix: Aim for 2–2.5L daily (more if active), including herbal teas. Pair with magnesium-rich foods, such as spinach, to gently hydrate the bowel without causing laxative dependence.
Fibre: Bulks, Softens, and Moves Stool
Soluble fibre (oats, psyllium, apples) draws water into stool, forming soft Type 3–4 sausages while stimulating peristalsis. Insoluble fibre (bran, veggies) adds bulk. Low fibre starves this process, leading to infrequent, pebble-like stools.
IBS Tip: Start low-FODMAP soluble sources (e.g. 5g psyllium husk daily with water) to avoid bloating while rebuilding regularity. Hydration is non-negotiable – fibre without water worsens constipation.
Caffeine: Laxative Effect with Loose Results
Coffee and tea stimulate colon contractions (like a mild laxative), speeding transit and producing looser Type 5–6 stools with higher water content. Great for constipation, but excess (>2 cups) risks diarrhoea or gut irritation.
Fix: Limit to 1 cup of black coffee/tea in the morning only; switch to dandelion root for motility without the crash.
Sugar Alcohols: Diarrhoea Triggers in “Healthy” Snacks
Sorbitol, xylitol, and mannitol (in gum, “sugar-free” bars, or low-carb treats) ferment undigested in the colon, pulling water in via osmosis. This creates urgent, watery Type 6–7 stools, a common IBS flare trigger.
Fix: Scan labels (avoid >2g/serving); use stevia or monk fruit instead. If diarrhoea hits, sip ginger tea and psyllium to bind excess water.
Quick Action Checklist
Track stool 3 days: note diet changes and Bristol type.
Test one tweak (e.g. +500ml water) and recheck in 48 hours.
Persistent issues? A diet alone may not resolve dysbiosis. Consider a stool test. Book Assessment
Optimising these keeps you in the ideal Type 3–4 zone for nutrient absorption and gut–brain calm
Keep yourself (and your poop) healthy
Healthy poop and a healthy you depend on many factors, including diet, exercise, overall health, medications, and stress. But lifestyle factors such as diet and exercise can go a long way toward producing perfect poo time after time.
FAQ: Common Poop Questions
How often should you poop? 3 times daily to 3 times weekly may be considered normal; less may indicate sluggish motility, while more may indicate fast transit due to inflammation, food hypersensitivities, allergens, and additives such as emulsifiers, among other factors.
What causes smelly stool?
Excess sulphur foods, not chewing food enough, poor digestion, or infections like H. pylori. Chronic stress (and anxiety) suppresses digestive capacities and is implicated in IBS-like symptoms, especially bloating and gas. If you eat too much in one sitting, don’t chew enough, drink too much liquid with the meal, it can also impact digestion, transit and fermentation, especially if you drink ultra-sweetened fizzy drinks with the meal (think meal deals in junk food outlets).
In some cases, foul-smelling faeces happen when your body is unable to process gluten or other nutrients. If you notice that your poop smells really bad after you eat certain things, it is time to check for food intolerances.
What does it mean when your poop sinks?
Poop sinks when it’s denser than water. Usually, this is a sign that your poop is normal and healthy. If your poop falls like a brick, you may have consumed mineral supplements, such as calcium or a mineral complex.
Is floating poop bad?
Stools often float because they are full of gas or excess fat (often due to a high intake of fatty foods, such as burgers/fried chicken, and chips). Greasy floating stools suggest malabsorption, especially if chronic. A warning sign to be careful of fat-soluble vitamins deficiency.
When does mucus in stool matter?
Occasional is fine; persistent signals inflammation or infection. People who are sensitive to gluten or dairy may notice mucus in their stools, especially if they are intolerant.
Why are my stools sometimes like tiny sausages and others like a very large sausage? When stressed, your colon is in “guarding” and may remain contracted for a long time, reducing the lumen (the inside of the tube) and leading to very thin, sausage-like stools. If you increase your intake of dietary fibre, you may see larger, well-formed stools that are easy to pass.
Do not underestimate the power of hydration.
Why do my bowel movements burn?
Anything that causes inflammation or irritation of the skin lining the rectum can cause burning when you have a bowel movement. Some of the most common causes of burning are:
Anal fissures (small tears)
Spicy food
Prolonged diarrhea
Constipation
Haemorrhoids
I spot blood on the toilet paper. What should I do?
Small amounts of bright‑red blood on toilet paper or pink water may indicate localised bleeding near the rectum. It may be due to haemorrhoids, but it may be more serious and require immediate medical attention.
Sometimes, eating pigmented foods, such as raw beetroot, may cause highly pigmented urine or the appearance of blood on the paper.
When a Functional Stool Test Makes Sense
If your stool shows types 1–2/5–7, odd colours, or the signs above persist despite diet tweaks, a comprehensive stool test can help reveal:
Pathogens (yeast, parasites, bacteria).
Dysbiosis ratios and inflammation markers.
Digestive enzymes, fat absorption, and short‑chain fatty acids.
Calprotectin for gut lining integrity (High levels are a sign of inflammation in your intestines. NICE endorses faecal calprotectin to differentiate IBD from IBS).
Unlike basic NHS tests, functional panels (such as GI Map or Comprehensive Stool Analysis) provide actionable insights for naturopathic protocols.
Culture vs PCR stool testing
Culture and PCR stool tests both look at what is in the stool, but they answer slightly different questions and are not interchangeable. The choice depends on the clinical context (acute infection vs. chronic gut issues, IBS vs. IBD, travel history, immune status, etc.).
Stool culture
Stool culture is the “classic” method used in hospitals for suspected infectious diarrhoea.
It involves growing live bacteria from the sample on selective media, then identifying them.
Standard culture panels usually focus on a small set of common pathogens such as Salmonella, Shigella, Campylobacter and some pathogenic E. coli.
Pros of stool culture
Proves viable organisms: You know the bug is alive and capable of infection, because it grows.
Allows antibiotic susceptibility testing: You can get a full antibiogram to guide targeted antibiotic choice for bacterial pathogens.
Cheaper per test than multiplex PCR in most public systems, especially if used selectively (e.g. only in severe or high‑risk cases).
Good for outbreak investigations: Public health labs still rely heavily on culture for typing and epidemiology (e.g. food‑borne outbreaks).
Cons of stool culture
Limited range of pathogens: Only a handful of bacteria are routinely looked for; most viruses and many parasites are missed unless specifically ordered.
Lower sensitivity: Many organisms are fastidious or present in low numbers and can be missed; overall detection rates are significantly lower than PCR panels.
Slow turnaround: Results can take 48–72 hours or more, delaying diagnosis and management.
Labour‑intensive: Requires manual plating and reading; this limits scalability and the breadth of organisms tested.
PCR stool testing
PCR‑based stool tests (often multiplex “GI panels,” “Gut Mapping”) detect DNA or RNA from pathogens in the sample. These are the tests we recommend in practice, as we need to know as much as possible about the communities in your gut. Culture testing, in this case, is insufficient.
A single multiplex PCR can simultaneously screen for a considerable number of pathogens (bacteria, viruses, and parasites) from a single stool specimen. As we learn more about new bacterial strains and research their impact on our health, PCR tests are becoming more comprehensive, incorporating them.
These tests do not require the organism to be alive; they detect genetic material.
Pros of PCR stool testing
Much higher sensitivity and detection rates. Multiplex PCR panels detect a substantially greater variety and number of pathogens than culture.
Broad pathogen coverage: Can identify viruses (e.g. norovirus, rotavirus), parasites (e.g. Giardia, Cryptosporidium), and less common bacteria that routine culture often misses.
Rapid results: Turnaround times can be hours rather than days (e.g., <3–4 hours vs. ~66 hours for culture).
Better clinical decisions in acute diarrhoea:
Higher detection rates lead to more accurate diagnosis of infectious vs. non‑infectious flares (e.g. in IBD or IBS) and fewer unnecessary endoscopies or steroid escalations.
Some studies show reduced antibiotic prescribing and health‑care utilisation when PCR panels are implemented.
Cons of PCR stool testing
Detects DNA, not just active infection: It may pick up:
Low‑level colonisation or prolonged shedding after a resolved infection.
Multiple organisms, some of which may be “bystanders”. This raises interpretation challenges and the risk of overdiagnosis.
Higher cost per assay: Multiplex PCR panels are usually significantly more expensive than basic culture.
Fixed target list: You detect only what the panel is designed to detect; emerging or unusual pathogens outside the panel will be missed. Always choose a well-established laboratory with comprehensive GI Mapping. These tend to provide more evidence-based answers and recommendations. Ask your practitioner if in doubt.
Ready for Personalised Gut Insights?
Book Your Stool Test Assessment
Book your consultation today and get a tailored stool test kit, analysis, and naturopathic plan for IBS, bloating, or gut health optimisation.
Sources
Guts Charity. (2025). What could your poo say about your health. Available at: https://gutscharity.org.uk/2024/08/what-your-poo-says-about-your-health [Accessed: 11 Feb. 2025]
NHS Forth Valley. (2025). Bristol Stool Chart Available at: https://nhsforthvalley.com/wp-content/uploads/2020/10/Bristol-Stool-Chart.pdf [Accessed: 12 Feb. 2025]
NHS UK. https://www.nhs.uk/symptoms/bleeding-from-the-bottom-rectal-bleeding
National Institute for Health Care Excellence (NICE).
References
Axelrad, JE., Freedberg, DE., Whittier, S. et al. (2019). Impact of gastrointestinal panel implementation on health care utilization and outcomes. Journal of Clinical Microbiology. 57(3), e01775-18. doi:10.1128/JCM.01775-18
Boeriu, A., Andone, A., Dobru, D. et al. (2025). PCR-based versus conventional stool testing in hospitalized patients with diarrhea: Diagnostic yield, clinical impact, and stewardship implications. Microorganisms. 13(12), 2785. doi:10.3390/microorganisms13122785
Chumpitazi, BP., Self, MM., Czyzewski, DI. et al. (2016). Bristol Stool Form Scale reliability and agreement decreases when determining Rome III stool form designations. Neurogastroenterology & Motility. 28(3), pp. 443-448. doi:10.1111/nmo.12738
Harvey, S. Matthai, S. King, DA. (2023). How to use the Bristol Stool Chart in childhood constipation. Archives of Disease in Childhood - Education and Practice. 108, pp. 35-339. doi:10.1136/archdischild-2022-324513
Hong, S., Zaki, TA., Main, M. et al. (2021). Comparative evaluation of conventional stool testing and multiplex molecular panel in outpatients with relapse of inflammatory bowel disease. Inflammatory Bowel Diseases. 27(10), pp. 1634-1640. doi:10.1093/ibd/izaa336
Macfarlane-Smith, LR., Ahmed, S., Wilcox, MH. (2018). Molecular versus culture-based testing for gastrointestinal infection. Current Opinion in Gastroenterology. 34 (1). pp. 19- 24. doi:10.1097/MOG.0000000000000405
Singh, V. Yune, P. Rasul, R. et al. (2020). 724. Gastrointestinal (GI) PCR vs stool cultures: Impact on length of hospital stay (LOS) and antibiotic use. Open Forum of Infectious Disease. 7(Suppl. 1), S412. doi:10.1093/ofid/ofaa439.916
Turgeon, DK., Fritsche, TR. (2001). Laboratory approaches to infectious diarrhea. Gastroenterology Clinics of North America. 30(3), pp. 693-707. doi:10.1016/s0889-8553(05)70206-5
Zhang, H. Morrison, S. Tang, YW. (2015). Multiplex polymerase chain reaction tests for detection of pathogens associated with gastroenteritis. Clinics in Laboratory Medicine. 35(2), pp. 461-486. doi:10.1016/j.cll.2015.02.006